

Abstract
Introduction
Daratumumab (DARA) is a human IgGκ anti-CD38 monoclonal antibody with a direct on-tumor and immunomodulatory mechanism of action. In combination with standard of care (SOC) regimens, DARA has consistently demonstrated a doubling of complete response (CR) rates, tripling of minimal residual disease (MRD)-negative rates, and reduction in the risk of progression or death by ≥50% vs SOC alone in relapsed/refractory MM and NDMM pts. In the prespecified interim analysis of ALCYONE, a phase 3 study of D-VMP versus VMP in transplant ineligible NDMM (Mateos MV, N Engl J Med 2018. 378[6]:518-528), significant progression-free survival (PFS) benefit (median not reached [NR] vs 18.1 mo; hazard ratio [HR], 0.50; P <0.001) and a higher rate of MRD negativity (10-5 threshold: 22% vs 6%; P <0.001) were observed without increased overall toxicity for D-VMP versus VMP after a median follow-up of 16.5 months. This report provides updated efficacy and safety findings from ALCYONE after 1 year of additional follow-up.
Methods
Pts were ≥65 years of age or ineligible for high-dose chemotherapy with autologous stem cell transplantation. Pts were randomized 1:1 to receive up to nine 6-week cycles of VMP (V 1.3 mg/m2 SC on Days 1, 4, 8, 11, 22, 25, 29, 32 [Cycle 1] and Days 1, 8, 22, and 29 [Cycles 2-9]; M 9 mg/m2 PO and P 60 mg/m2 PO on Days 1-4 [Cycles 1-9]) with or without DARA (16 mg/kg IV QW for Cycle 1, Q3W for Cycles 2-9, and Q4W for Cycles 10+ until disease progression). PFS was the primary endpoint. PFS on the subsequent line of therapy (PFS2), overall response rate (ORR), CR or better rate, very good partial response (VGPR) or better rate, MRD-negative rate (10-5 threshold: clonoSEQ® V2.0, Adaptive), overall survival (OS), and safety were secondary endpoints. PFS2 was defined as the duration from randomization to progression on the next line of subsequent antimyeloma therapy or death, whichever occurred first.
Results
A total of 706 pts were randomized (350 D-VMP; 356 VMP). Median (range) age was 71 (40-93) years, with 29.9% being ≥75 years of age. Of the 616 pts evaluable for cytogenetic risk assessment via fluorescence in-situ hybridization/karyotyping, 84.1% had standard-risk and 15.9% had high-risk (del17p, t[14;16], and/or t[4;14] positive) disease. At the updated clinical cutoff date (June 12, 2018), all pts in both arms had either completed or discontinued from 9 treatment cycles of VMP, with 194 (56%) pts in the D-VMP arm remaining on the study to receive DARA monotherapy in Cycles 10+.
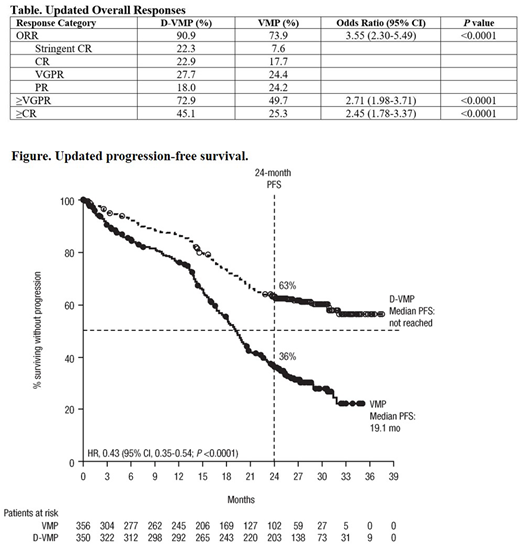
After median follow-up of 27.8 months, median PFS was NR for D-VMP vs 19.1 months for VMP (HR, 0.43; 95% confidence interval [CI], 0.35-0.54; P <0.0001; Figure). All prespecified subgroups showed a PFS benefit of D-VMP vs VMP, including pts ≥75 years of age (median: 32.2 mo vs 20.1 mo; HR, 0.51; 95% CI, 0.34-0.75). Significantly higher ORR and rates of deeper responses were observed for D-VMP vs VMP (Table). Median duration of response among responders was NR for D-VMP vs 21.1 months for VMP. Median PFS2 was NR in either arm (unstratified HR, 0.59; 95% CI, 0.43-0.82; P = 0.0013); 24-month PFS2 rates were 84.1% vs 78.5%, respectively. Updated MRD results will be presented.
Grade 3/4 treatment-emergent adverse events (TEAEs; D-VMP/VMP) occurring in ≥10% of pts were neutropenia (39.9%/39.0%), thrombocytopenia (34.7%/37.9%), anemia (17.1%/19.8%), and pneumonia (12.4%/4.0%); grade 3/4 infection rates were 25.1% vs 14.7%, respectively. Among D-VMP pts who received D monotherapy (Cycles 10+; n = 278), 66 (23.7%) pts reported grade 3/4 TEAEs; the most common were anemia (3.6%), pneumonia (2.5%), neutropenia (1.8%), and thrombocytopenia (1.4%). Two pts in the D-VMP arm and 1 pt in the VMP arm discontinued treatment due to pneumonia, and treatment discontinuations due to infection occurred in 1.4% vs 1.7% for D-VMP vs VMP.
Conclusions
With 1 year of additional follow-up, the combination of DARA and VMP in transplant ineligible NDMM pts continues to demonstrate a significant PFS benefit, including in pts ≥75 years of age, and allows for maintenance of PFS benefit during the subsequent line of therapy. Improvements in duration and depth of response continue to be observed with D-VMP with longer follow-up. No new safety signals emerged following the addition of DARA to VMP, and grade 3/4 infections continue to be manageable with no notable increase in rates. These results continue to support the use of D-VMP in the first line of treatment in transplant ineligible NDMM.
Dimopoulos:Amgen: Honoraria; Bristol-Myers Squibb: Honoraria; Janssen: Honoraria; Celgene: Honoraria; Takeda: Honoraria. Mateos:GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Cavo:Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Bristol-Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees; GlaxoSmithKline: Honoraria, Membership on an entity's Board of Directors or advisory committees. Suzuki:Sanofi Aventis: Consultancy, Honoraria; Ono: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; SRL.Inc: Employment. Jakubowiak:Bristol-Myers Squibb: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Karyopharm: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria; Adaptive Biotechnologies: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; SkylineDx: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria. Knop:Takeda: Consultancy, Honoraria, Research Funding; Bristol Myers Squibb: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding. Doyen:Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees. Lucio:Janssen: Consultancy, Honoraria, Speakers Bureau; Celgene: Consultancy, Honoraria, Speakers Bureau; Takeda: Consultancy, Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Speakers Bureau. Cook:Chugai: Honoraria; Janssen: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Jazz: Honoraria; YAkeda: Honoraria; Amgem: Honoraria. Grosicki:Affimed: Research Funding. Garg:Novartis: Other: travel support, Research Funding; Janssen: Honoraria; Takeda: Other: Travel Grant; Amgen: Honoraria, Other: Travel Support. Chiu:Janssen Research & Development, LLC: Employment. Wang:Janssen Research & Development, LLC: Employment. Kudva:Janssen Research & Development: Employment. Kobos:Janssen Research & Development: Employment. Wroblewski:Janssen Research & Development: Employment. Qi:Janssen Research & Development, LLC: Employment. San-Miguel:Celgene: Honoraria; Sanofi: Honoraria; Novartis: Honoraria; BMS: Honoraria; Amgen: Honoraria; Janssen: Honoraria; Roche: Honoraria. Bladé:Janssen: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal